Nurse Practitioner Career Guide USA 2026: Salary, Path & Honest ROI
Updated May 14, 2026 • Reading Time: ~23 Minutes
The US Bureau of Labor Statistics projects that nurse practitioner jobs will grow 40 percent between 2024 and 2034 – ten times the average for all occupations. The median NP salary sits at $129,210, roughly 38 percent above what the median registered nurse earns. US News & World Report ranked nurse practitioner the number one job in healthcare for 2026. On paper, the case looks closed: become an NP.
The reality is more textured. NP education costs real money – anywhere from $25,000 to over $100,000. The salary advantage varies enormously by specialty, by state practice law, and by whether you work in primary care or a hospital. A Family Nurse Practitioner in a saturated metro market is not in the same financial position as a Psychiatric-Mental Health NP running an independent practice in a full practice authority state. And the question of whether you need a master’s or a doctorate has a clearer answer than most program brochures suggest.
This guide covers the whole NP picture for 2026 – the pathway, the specialties and what each pays, the state-by-state practice authority map, certification, and an honest return-on-investment analysis. Verified figures from the BLS, the American Association of Nurse Practitioners, and NCSBN. Written for the RN who is seriously weighing whether advanced practice is the right next move.
🩺 The Nurse Practitioner Picture – 2026 Verified Data
Median NP salary: $129,210 (BLS, May 2024 data)
Salary range: ~$97,960 (10th percentile) to ~$169,950+ (90th)
Job growth 2024–2034: 40% (BLS) – 10x the all-occupation average
Annual openings (NP/CRNA/CNM combined): ~32,700/year
NPs practicing in the US: 461,000+ (2025)
Full practice authority: 27 states + DC (April 2026)
Degree required: MSN minimum (DNP optional, not mandated)
Time to become an NP (from BSN): 2–4 years
Education cost: ~$25,000–$100,000+
Table of Contents
- What a Nurse Practitioner Actually Does
- The Pathway: RN to NP, Step by Step
- MSN or DNP? The Honest Answer
- The Specialties – and What Each Pays
- Full Practice Authority: The State Map That Shapes Your Career
- Certification and Licensing
- The Cost and the Honest ROI
- What the Brochures Don’t Tell You
- Is the NP Path Right for You?
- Frequently Asked Questions
1. What a Nurse Practitioner Actually Does
A nurse practitioner is an Advanced Practice Registered Nurse (APRN) – a registered nurse with graduate-level education who can evaluate patients, diagnose conditions, order and interpret diagnostic tests, develop treatment plans, and prescribe medications. In much of the country, an NP does clinically what people traditionally associate with a physician’s role in primary care.
NPs are one of four APRN roles, alongside Certified Registered Nurse Anesthetists (CRNAs), Certified Nurse Midwives (CNMs), and Clinical Nurse Specialists (CNSs). Of the four, NPs are by far the largest group – more than 461,000 were practicing in the US in 2025, delivering an estimated 1.06 billion patient visits a year.
The role exists because of a real structural gap. The first NP program was created in 1965 at the University of Colorado, in direct response to a primary care physician shortage that followed the expansion of Medicare and Medicaid. Sixty years later, the same pressure is driving the profession’s growth: an aging population, a projected physician shortfall the Association of American Medical Colleges has estimated in the tens of thousands, and a mental health crisis with nowhere near enough prescribers. NPs have moved from the margins of healthcare delivery to its center.
What an NP does day to day depends heavily on specialty and setting. A Family NP in a primary care clinic manages chronic disease, treats acute illness, and handles preventive care across all ages. A Psychiatric-Mental Health NP diagnoses and medicates psychiatric conditions. An Acute Care NP works in hospitals and ICUs. The credential is the same category; the work is not interchangeable.

2. The Pathway: RN to NP, Step by Step
There is no shortcut directly into the NP role. You become a registered nurse first, then build on that. The standard pathway:
Step 1 – Become a registered nurse. Earn an ADN or BSN and pass the NCLEX-RN. A BSN is the smoother route because most NP programs require it for admission. If you have an ADN, you will either complete a BSN or enter an RN-to-MSN bridge program that folds the bachelor’s-level coursework into the graduate pathway.
Step 2 – Gain RN clinical experience. Most NP programs expect at least 1 to 2 years of RN experience, and many competitive programs prefer more. Beyond admissions, this experience matters for the work itself – advanced practice builds on clinical judgment that only develops at the bedside. Experience in the field related to your intended specialty strengthens both your application and your eventual practice.
Step 3 – Choose your specialty and population focus. This is a more consequential decision than many nurses realize, because your NP certification is tied to a specific patient population. An FNP cannot simply switch to treating psychiatric patients later; that requires a separate post-master’s certificate. Choose deliberately. (Section 4 covers the specialties in detail.)
Step 4 – Complete a graduate NP program. Either an MSN (2–3 years) or a DNP (3–4 years), accredited by the Commission on Collegiate Nursing Education (CCNE) or the Accreditation Commission for Education in Nursing (ACEN). NP programs combine graduate coursework – advanced pathophysiology, advanced pharmacology, advanced health assessment, and specialty content – with supervised clinical hours. Expect 500 to 700+ clinical hours depending on the program and specialty.
Step 5 – Pass national certification. After graduating, you sit for a national certification exam in your specialty, administered by a body such as the American Association of Nurse Practitioners Certification Board (AANPCB) or the American Nurses Credentialing Center (ANCC).
Step 6 – Obtain state APRN licensure. With your certification, you apply to your state board of nursing for an APRN license and, separately in many states, for prescriptive authority and a DEA registration to prescribe controlled substances.
The realistic total timeline: from the start of nursing school to practicing as an NP is generally 6 to 8 years – undergraduate nursing education, RN experience, and graduate study combined. For a nurse who already holds a BSN and RN experience, the remaining NP-specific portion is 2 to 4 years.
For the foundational degree decision that comes first, see ADN vs BSN: Which Nursing Path Is Better in 2026 and Best Online RN-to-BSN Programs 2026.
3. MSN or DNP? The Honest Answer
This is the decision NP applicants agonize over, and the marketing around it muddies the water. Here is the straightforward version.
The MSN (Master of Science in Nursing) is the current minimum degree required to become a nurse practitioner. It takes 2 to 3 years, focuses on the clinical preparation you need for your specialty, and qualifies you to sit for certification and enter practice.
The DNP (Doctor of Nursing Practice) is a terminal practice doctorate. It takes 3 to 4 years and adds substantial coursework in healthcare systems, leadership, health policy, quality improvement, and translating research into practice. It also qualifies you for NP certification and practice.
Here is the part the brochures soften: the DNP is not required to become or work as a nurse practitioner. The American Association of Colleges of Nursing recommended back in 2004 that the DNP become the entry-level degree for advanced practice, and that recommendation has been discussed for two decades – but it has never been adopted as a licensure requirement. As of 2026, you can have a full, well-paid NP career with an MSN.
So who should choose which?
Choose the MSN if: your goal is clinical practice, you want to start earning an NP salary sooner, cost is a real consideration, or you are not certain you want the leadership and systems focus the DNP adds. The MSN is the faster, cheaper route into the same clinical role. You can always complete a post-master’s DNP later, often while working as an NP.
Choose the DNP if: you want to move into health system leadership, academic faculty roles, or health policy; you are drawn to the quality-improvement and systems content; or you simply want the terminal degree and have the time and resources for it. In some competitive markets and academic settings, the DNP carries weight.
What the DNP generally does not do is produce a large clinical salary premium on its own. A DNP-prepared FNP and an MSN-prepared FNP doing the same primary care job are often paid similarly. Pay is driven more by specialty, setting, state, and experience than by the master’s-versus-doctorate distinction. Decide based on the career you want, not on an assumption that the doctorate automatically pays for itself.
4. The Specialties – and What Each Pays
Your NP specialty is defined by patient population, and it shapes both your daily work and your earning potential. The major specialties:
| Specialty | Patient Focus | Indicative Median Pay |
|---|---|---|
| Family NP (FNP) | All ages, primary care | ~$128,000 |
| Psychiatric-Mental Health NP (PMHNP) | Mental health, all ages | $139,000+ |
| Neonatal NP (NNP) | Newborns, NICU | $139,000+ |
| Acute Care NP (ACNP / AGACNP) | Hospital, critical care | ~$117,000–$135,000 |
| Adult-Gerontology Primary Care NP (AGPCNP) | Adults and older adults | ~$120,000–$128,000 |
| Pediatric NP (PNP) | Infants through young adults | ~$125,000–$135,000 |
| Women’s Health NP (WHNP) | Reproductive, gynecologic health | ~$115,000–$125,000 |
Pay figures are indicative medians synthesized from BLS Occupational Employment data and AANP workforce survey reporting. Actual salaries vary widely by state, setting, and experience. The overall BLS median across all NP specialties is $129,210.
The FNP reality
The Family Nurse Practitioner is the most common specialty by a wide margin – and that popularity is exactly why FNP pay sits near the overall median rather than above it. In some metropolitan markets, FNP supply has caught up with demand, and new-graduate FNPs report genuine competition for jobs and softer starting offers. FNP is versatile and the broadest in scope, but “most common” and “highest-paid” are not the same thing.
Why PMHNP keeps topping the pay tables
The Psychiatric-Mental Health NP is consistently among the highest-earning and fastest-growing NP specialties, and the reason is straightforward supply and demand. The US has a severe shortage of psychiatric prescribers. PMHNPs help fill that gap, and in full practice authority states a PMHNP can run an independent psychiatric practice. The specialty also offers more telehealth flexibility than most clinical roles, since psychiatric evaluation and medication management translate well to remote care. For an RN choosing a specialty primarily on earning potential and job security, PMHNP has the strongest current case.
For a broader look at how nursing specialties compare on pay, see Nursing Specialty Salaries 2026.
5. Full Practice Authority: The State Map That Shapes Your Career
Where you practice as an NP matters as much as what specialty you choose – because state law determines how independently you can work. The American Association of Nurse Practitioners defines three practice environments:
Full practice authority. State law permits NPs to evaluate, diagnose, order and interpret tests, and initiate and manage treatment – including prescribing medications and controlled substances – under the exclusive licensure authority of the state board of nursing. No physician collaboration agreement is required. As of April 2026, 27 states plus Washington DC grant full practice authority. This is the model endorsed by the National Academy of Medicine and NCSBN.
Reduced practice. State law reduces NP practice in at least one element, typically requiring a career-long collaborative agreement with a physician for the NP to deliver some part of patient care.
Restricted practice. State law requires career-long physician supervision, delegation, or team management for the NP to practice at all.
Why this matters financially and practically: in a full practice authority state, an NP can open an independent practice with no physician on the payroll. In a reduced or restricted state, a collaborating physician’s signature is a requirement – and that collaboration often carries a real ongoing cost, sometimes tens of thousands of dollars a year, paid by the NP or the practice for what can amount to a signature and periodic chart review. Two NPs with identical credentials and identical patients can have very different overheads depending purely on the state line they practice on.
The trend has run steadily toward full practice authority for three decades – from five states in 1994 to 27 plus DC in 2026 – but the remaining states include some of the largest healthcare markets, and change there has been slow and politically contested. If independent practice is part of your long-term plan, your state’s practice authority status belongs near the top of your decision factors. The AANP maintains a current State Practice Environment map; verify your specific state before making plans, as legislation moves year to year.
6. Certification and Licensing
After you complete your NP program, two things stand between you and practice: national certification and state licensure.
National certification. You sit for a certification exam specific to your population focus. The two largest certifying bodies are the American Association of Nurse Practitioners Certification Board (AANPCB) and the American Nurses Credentialing Center (ANCC). Which one you use depends on your specialty – for example, FNP and adult-gerontology primary care certifications are offered by both, while PMHNP certification is offered through ANCC. Certification is time-limited and maintained through continuing education and practice hours.
State APRN licensure. With your certification in hand, you apply to your state board of nursing for an APRN license. Many states issue prescriptive authority separately, and you will also need a federal DEA registration to prescribe controlled substances. Licensing fees typically run $100 to $500, and processing can take weeks to a few months depending on the state and how quickly you supply documentation.
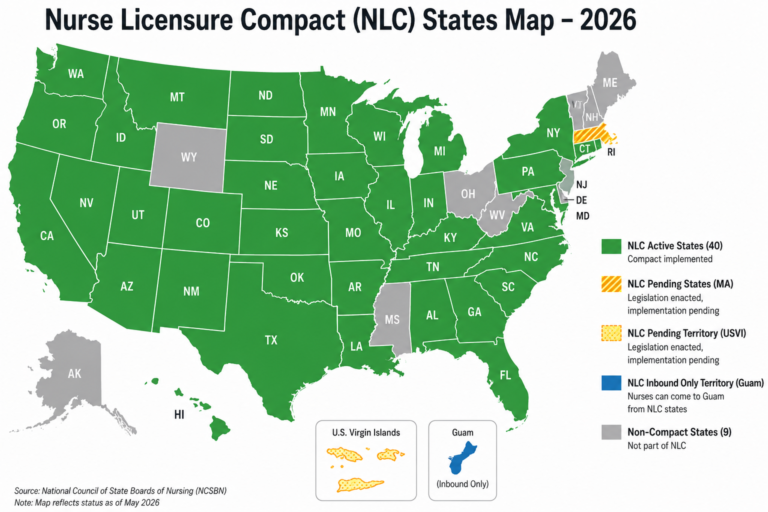
If you move states – and many NPs do – expect to re-license in the new state, verify your RN license through Nursys, have your certifying body confirm your NP certification, and potentially apply for new prescriptive authority and update your DEA registration. The APRN Compact, which would streamline multi-state practice the way the existing RN Nurse Licensure Compact does, has been enacted into law by a number of states but is not yet operational nationally. Until it activates, NP licensure remains a state-by-state process.
7. The Cost and the Honest ROI
NP education is an investment, and like any investment it deserves an honest accounting rather than a brochure figure.
What it costs
NP program tuition varies widely. A public university MSN for an in-state student can run roughly $25,000 to $50,000. A private university or a DNP program can reach $80,000 to $100,000 or more. Add the indirect costs: textbooks and fees, certification exam fees, licensing fees, and – the one most applicants underestimate – the income reduction during clinical rotations, when many students cut back their RN hours to complete unpaid clinical placements.
What it returns
The median NP earns $129,210; the median RN earns $93,600. That is a gap of roughly $35,600 a year. Against an MSN costing, say, $40,000, the arithmetic is favorable – the education cost is recovered within two to four years of practicing as an NP, and the higher salary continues for the rest of your career.
That is the case for the NP path, and for many nurses it genuinely holds. But the honest version includes the qualifiers:
The gap is a median, not a guarantee. A new-graduate FNP in an oversupplied metro market may start well below $129,210. The salary advantage is real on average and over a career, but it is not instant and not uniform.
Existing debt changes the math. If you are already carrying significant RN-era student loans, adding $40,000 to $100,000 of graduate debt is a different decision than starting from zero. Run your actual numbers, not the average.
Employer tuition support changes everything. Many hospital systems offer tuition reimbursement for NP education, sometimes substantial, often with a service commitment. An NP degree subsidized by an employer has a dramatically better ROI than one financed entirely with loans. Investigate this before you enroll.
Specialty and state swing the outcome. A PMHNP in a full practice authority state and a WHNP in a restricted state who paid private-school tuition are looking at very different returns on the same category of degree.
The honest summary: for most committed RNs, becoming an NP is financially worth it – the career-long salary differential outweighs the education cost. But it is not automatically worth it for every nurse in every situation, and “NPs earn six figures” is not by itself a financial plan. Do the calculation with your real debt, your real target specialty, and your real state.
For help managing the debt side of this equation, see Student Loan Repayment for Nurses 2026 – several forgiveness programs apply to NPs in qualifying settings.
8. What the Brochures Don’t Tell You
Every NP program website emphasizes the salary and the autonomy. Here are the things that matter just as much and get far less airtime.
Finding your own clinical placements can be brutal. Many NP programs – especially online ones – require students to source their own preceptors and clinical sites. In saturated markets, securing 600+ hours of quality preceptorship is genuinely difficult, and a weak placement undermines your education. Before enrolling, ask the program directly: do you place students, or am I on my own? The answer should weigh heavily.
The transition from RN to NP is its own reality shock. Being an excellent bedside nurse does not automatically make the leap to diagnostician and prescriber feel natural. The first year as a new NP carries a steep confidence curve, much like the first year as a new RN. Programs and employers vary widely in how much new-NP support they offer.
FNP market saturation is real in some regions. The FNP is the most-produced NP credential, and in certain metro areas supply has caught up with demand. This does not mean the NP path is closed – it means specialty choice and geographic flexibility matter. PMHNP, acute care, and willingness to work in underserved or rural areas all improve the picture considerably.
Collaboration agreements cost money in non-FPA states. If you practice in a reduced or restricted state, the required physician collaboration is not free. NPs in these states sometimes pay a physician thousands of dollars annually for the collaborative relationship. Factor it in.
Productivity pressure is part of the job. Many NP roles, particularly in primary care, come with patient-volume expectations – a set number of encounters per day. The autonomy of the NP role is real, but so is the throughput pressure of modern healthcare. The job is rewarding; it is not relaxed.
9. Is the NP Path Right for You?
Strip away the salary headlines and ask yourself these questions honestly.
Do you want to diagnose and prescribe, or do you love bedside nursing? The NP role is a genuine change of work, not just a pay raise. Some of the best RNs are happiest at the bedside and would not enjoy the diagnostic, documentation-heavy reality of advanced practice. There is no shame in that – but be honest about which work you actually want.
Can you commit 2 to 4 more years of study while likely still working? Most NP students work as RNs through their program. It is demanding. Family circumstances, finances, and energy all factor in.
Have you chosen your specialty deliberately? Because the certification is population-specific, this choice is hard to undo. Spend real time on it. Shadow NPs in the specialties you are considering if you can.
Does your state’s practice environment match your goals? If you dream of independent practice, a restricted state will frustrate that dream – or require relocation.
Have you run your own ROI, not the average one? Your debt, your target specialty, your state, your employer’s tuition support. The median is a starting point, not your answer.
For the nurse who wants more clinical autonomy, is genuinely drawn to diagnosis and treatment, chooses a specialty with strong demand, and runs the numbers with clear eyes – the NP path is one of the strongest career moves available in healthcare today. The 40 percent growth projection and the number-one-job ranking are not marketing inventions; they reflect a real, durable need. Just make the decision as the informed professional you already are.
10. Frequently Asked Questions
How much do nurse practitioners earn in 2026?
Median $129,210 per year (BLS, May 2024 data). Range roughly $97,960 to $169,950+. PMHNPs and NNPs lead at $139,000+. California pays the highest state median. NPs earn about 38% more than the median RN.
How long does it take to become an NP?
From a BSN: 2–3 years via MSN, 3–4 via DNP. From an ADN: add 1–2 years for a BSN or RN-to-MSN bridge. Full pathway from starting nursing school: 6–8 years.
What is the NP job outlook?
BLS projects 40% growth for NPs, nurse anesthetists, and nurse midwives from 2024–2034 – about 10x the all-occupation average. Roughly 32,700 combined openings per year. NP is ranked the #1 healthcare job by US News.
MSN or DNP?
The MSN is the minimum required and is faster and cheaper. The DNP adds leadership, systems, and policy content over 3–4 years but is not required for NP licensure. The DNP rarely produces a clinical salary premium on its own. Choose based on whether you want leadership/academic roles.
What are the main NP specialties?
FNP (all ages, most common), PMHNP (mental health, highest-paid), AGNP (adults/older adults), PNP (children), NNP (newborns), WHNP (women’s health), ACNP (acute/hospital care). Certification is population-specific.
What is full practice authority?
State law letting NPs evaluate, diagnose, test, treat, and prescribe independently – no physician collaboration agreement. 27 states + DC as of April 2026. Other states require reduced or restricted practice.
Is becoming an NP worth the cost?
For most committed RNs, yes. Education runs ~$25,000–$100,000+; the NP-RN salary gap is ~$35,600/year, recovering an MSN’s cost within 2–4 years. But it depends on your debt, specialty, state, and employer tuition support. Not automatically worth it for everyone.
Do I need a BSN?
Most NP programs require it, but RN-to-MSN bridge programs accept ADN-prepared nurses, adding 1–2 years. A current RN license is required before any NP program.
Which specialty pays the most?
PMHNP and NNP, both with medians above $139,000. PMHNP has the strongest current case due to the psychiatric prescriber shortage and telehealth flexibility.
Can NPs open their own practice?
In the 27 full practice authority states plus DC, yes – fully independent. In reduced/restricted states, a physician collaboration agreement is required, which carries ongoing cost.
The Bottom Line
Nurse practitioner is, by the numbers, one of the best career moves in American healthcare in 2026 – a $129,210 median, 40 percent projected growth, and a structural shortage of providers that is not closing any time soon. The profession has moved from the edge of healthcare to its center, and the trend lines all point the same direction.
But “best career move on average” is not the same as “right for you automatically.” The NP role is a genuine change of work, the education costs real money and time, the FNP market is saturated in places, and your state’s practice laws can quietly shape your entire career. The nurses who thrive as NPs are the ones who chose the path deliberately – the right specialty, a clear-eyed ROI calculation, a realistic view of the work – rather than the ones who chased a salary headline.
If you have read this far and the work itself still appeals to you – the diagnosing, the prescribing, the autonomy, the deeper clinical responsibility – then the NP path is very likely worth pursuing. Choose your specialty with care, check your state, run your real numbers, and go.
Related articles on GlobalNurseGuide.com:
ADN vs BSN: Which Nursing Path Is Better in 2026?
Best Online RN-to-BSN Programs 2026
Nursing Specialty Salaries 2026: What Every Specialty Pays
Student Loan Repayment for Nurses 2026
Highest-Paying Nursing Jobs 2026
Nursing Class of 2026: Your First 30 Days as a New RN
Nursing Jobs in USA 2026: Ultimate Guide
Disclaimer:
This article is for informational purposes only and does not constitute career, financial, or educational advice. Salary figures, job growth projections, practice authority classifications, and program costs are subject to change. Salary and employment data sourced from the US Bureau of Labor Statistics (BLS) Occupational Employment and Wage Statistics and Occupational Outlook Handbook (May 2024 data, 2024–2034 projections). Practice authority data sourced from the American Association of Nurse Practitioners (AANP) State Practice Environment map, current as of April 2026. NP workforce figures from AANP. Always verify current requirements with your state board of nursing, your chosen accredited program, and the relevant certification body (AANPCB or ANCC) before making decisions. Indicative specialty pay ranges synthesize BLS and AANP data and vary by location, setting, and experience. GlobalNurseGuide.com is not affiliated with any educational institution, certification body, or government agency. Information current as of May 14, 2026.
© 2026 GlobalNurseGuide.com – Empowering Nurses Worldwide with Real Opportunities
Author

Discover more from Global Nurse Guide
Subscribe to get the latest posts sent to your email.