US Nursing Shortage 2026: Which States Are Hiring the Most RNs This Spring
If you have been paying attention to the nursing job market lately, you already know demand is strong. What you may not know is how dramatically it varies from state to state – and why that difference matters enormously for every career decision you make this year.
The national numbers tell one story. Right now, the Health Resources and Services Administration (HRSA) estimates there are currently 263,870 open registered nurse positions nationwide, and that number is not going down any time soon. The Bureau of Labor Statistics projects approximately 189,100 RN openings per year through 2034, driven by both workforce turnover and an aging population that is steadily requiring more care.
But national averages are misleading when you are the one deciding where to work, whether to pursue further education, or how hard to push in a salary negotiation. The real story – the one that actually affects your paycheck, your commute, and your quality of life as a nurse – is playing out differently in every state, and in many cases, in every county.
🩺 Going to the US as a nurse?
Get weekly vacancy alerts, EB-3 visa updates & daily NCLEX prep on WhatsApp — FREE.
📲 Follow the ChannelThis spring, the gap between where nurses are needed most and where they are most plentiful is wider than it has been in years. Here is what the data actually shows – and what it means for nurses thinking about their next move.
The National Picture, Honestly
Before diving into the state-by-state breakdown, it helps to understand the two forces running in opposite directions at the same time.
On one hand, the overall nursing workforce has been growing. More people are becoming nurses than at any point in the profession’s history, and nursing school enrollment – despite ongoing capacity problems – is higher than it was five years ago.
On the other hand, demand is growing faster. Rural and non-metropolitan areas face a 22% shortage in 2026, compared to an 8% shortage in metro regions. That rural-urban divide is not a footnote. It is the defining feature of the nursing shortage in 2026, and it shapes everything from travel nursing rates to the geographic distribution of sign-on bonuses.
The other structural reality bearing down on the market this spring: over one million RNs are projected to retire by 2030, and as of 2022, 23% of RNs working in outpatient settings have either already retired or are set to retire within five years. The wave is not coming – it is already here. The nurses leaving right now are the experienced ones, the charge nurses, the preceptors, the people who held institutional knowledge that cannot be easily replaced. That is a different kind of shortage than simply not having enough bodies in scrubs.

The States With the Sharpest Shortages This Spring
California – The Largest Absolute Deficit in the Country
California is expected to be short the most registered nurses of any state – approximately 45,500 – nearly three times the deficit of the next most affected state. That number is staggering on its own. What makes it more complicated is that California is simultaneously one of the highest-paying states for nurses in the country. The state’s mandatory staffing ratios, stronger than anywhere else in the US, mean hospitals cannot quietly absorb the shortage by simply stretching existing staff thinner. When they are short nurses, they are genuinely short – positions go unfilled or are filled with agency staff at significant cost.
For nurses considering California, the picture is this: the jobs are there, the pay is real (California offers some of the highest gross RN salaries in the country, with OR nurses averaging around $110,000 annually), and the working conditions – particularly in unionised facilities – are generally stronger than in most other states. The catch is cost of living, which significantly erodes the purchasing power of that salary depending on where in the state you land. Nurses who choose to live 60 to 90 miles from the major metro areas, while working in them, often find the financial arithmetic considerably more favourable.
In California, as many as 20% of all OR nurses are set to retire in the next five years, which means the specialty pipeline is particularly strained right now and the competition for experienced perioperative nurses is fierce.
Georgia – Aggressive Hiring in Atlanta, Crisis in Rural Areas
Georgia deserves more attention in the national nursing conversation than it typically gets. Georgia has 21% fewer registered nurses than it needs according to HRSA data, and the state is expected to see the second-highest estimated shortage among all US states by 2035.
The Atlanta metro area is one of the most actively hiring healthcare markets in the country right now. Major systems – Emory Healthcare, Piedmont, WellStar, and Grady – are competing directly for experienced RNs and offering sign-on packages to attract candidates. Analysis of 2026 healthcare migration trends shows a supply deficit in the Atlanta metro region, with major hospital systems such as Emory and Piedmont competing aggressively for staff.
The rural situation in Georgia is considerably more difficult. The shortage is felt most acutely in rural areas, partly due to the pay gap: registered nurses in metro Atlanta earn an average of $77,000 per year, while those in southwest Georgia earn $62,800. That $14,000 annual gap is the central reason rural Georgia hospitals struggle to attract nurses when Atlanta is an hour or two away offering better pay, more clinical opportunities, and generally more developed support infrastructure.
For nurses drawn to Georgia, the metro areas offer solid career momentum right now. For nurses who specifically want rural practice – and some genuinely do, for the breadth of practice and pace of life – the shortage conditions there translate into real negotiating leverage, often including loan forgiveness, housing stipends, and faster advancement timelines than you would see at a large urban system.
Texas – Second-Largest Absolute Shortage, Strong Salary Growth
Texas is the second most affected state by raw numbers, with HRSA projecting that Texas will need to add approximately 88,800 new registered nurse positions by 2030 – and that growth alone will not be enough to close the existing gap.
The state’s healthcare market is defined by its sheer geographic spread and demographic growth. The major metros – Houston, Dallas-Fort Worth, San Antonio, and Austin – each have their own distinct hiring dynamics, and all of them are actively recruiting. The average RN salary in Texas is approximately $41.65 per hour based on active job market data, which translates to a competitive annual salary when combined with the state’s lack of income tax – a meaningful financial advantage that nurses moving from high-tax states often underestimate.
Relocation packages in Texas are becoming increasingly common. Active job postings for major hospital systems in Houston and San Antonio include relocation bonuses of up to $15,000 for candidates relocating from out of state, alongside standard sign-on bonuses in the $5,000 to $20,000 range for specialty positions.
Idaho – The Most Severe Shortage Rate in the Country
The headlines about California and Texas are understandable – the absolute numbers are large – but Idaho is the state with the most structurally severe shortage when measured as a proportion of what the state actually needs. Idaho had an expected shortage of 38% in 2025, meaning the state was meeting only about 62% of its RN demand. That figure is expected to improve to around 17% by 2037, but the road between here and there is long and, for working nurses in the state right now, it means conditions that are consistently strained.
Rural Idaho is particularly difficult. For experienced nurses willing to work in smaller facilities and take on the expanded scope that rural practice often requires, the combination of shortage conditions and federal loan forgiveness programmes – particularly through the HRSA Nurse Corps programme, which prioritises Health Professional Shortage Areas – can make a genuine financial case for rural Idaho positions that is not immediately obvious from salary figures alone.
States like Idaho, New Mexico, and Virginia have some of the lowest nurse-to-population ratios in the country, suggesting that facilities in these areas face additional challenges including longer wait times, difficulty maintaining safe workloads, and increased nurse fatigue from unmanageable workflows.
Washington, North Carolina, and Michigan – Worsening Conditions
Three states that do not always make the top of shortage lists but are seeing significant deterioration this spring: Washington, North Carolina, and Michigan.
HRSA identified the biggest projected RN shortages as being concentrated in Washington, Georgia, California, Oregon, Michigan, Idaho, Louisiana, North Carolina, New Jersey, and South Carolina.
North Carolina is notable because its trajectory is running the wrong direction. North Carolina has an anticipated shortage of 15% in 2025, rising to 22% by 2037 – one of the few states where the shortage is projected to substantially worsen rather than stabilise over time. The state’s nursing schools are working to expand capacity, but the population growth in the Charlotte and Research Triangle areas is outpacing the training pipeline.
In Michigan, a late 2024 survey from the Michigan Health Council found that 32% of Michigan RNs reported intentions to leave the profession or their current role within the next 12 months, primarily due to burnout and workplace safety concerns. That level of anticipated attrition, if even half of it materialises, will create acute vacancies in a state that already has limited excess nursing supply.
The States That Are Hiring – But for Different Reasons
There is an important distinction worth making between states with shortages and states that are actively hiring at scale right now. Those two things are related, but they are not identical.
Some states – Florida is the clearest example – have complex dynamics worth understanding before you assume a surplus means fewer opportunities.
Florida – More Complicated Than the Numbers Suggest
Florida is projected to have the most extra nurses of any state – a surplus of approximately 53,700 – the largest overage in the country. At first read, that sounds like Florida is not a strong market for nursing employment. The reality is more nuanced.
Florida’s surplus is concentrated in certain metro areas and certain nursing types. The state still has active nursing hiring because of its enormous population base, its high proportion of elderly residents requiring complex care, its rapid regional population growth in areas like the Tampa Bay corridor and Space Coast, and significant internal turnover within the nursing workforce itself.
National RN turnover remains elevated, with hospitals hiring roughly 385,000 RNs to backfill positions and cover growth annually. In a state as large as Florida, that churn alone sustains a significant hiring market, even in areas that show net supply surplus at the aggregate level.
The practical guidance for nurses considering Florida: the market is active, but it is not as straightforward as shortage states where almost any credentialed RN is aggressively recruited. Nurses with specialty certifications – OR, ICU, labour and delivery, emergency – have considerably stronger positioning than general med-surg candidates.
The Rural-Urban Divide: The Story Inside the Story
One number that does not get enough attention in mainstream nursing coverage is this: rural areas face a 22% nursing shortage in 2026, compared to an 8% shortage in metro regions.
That is not a minor variation. It means rural American healthcare is nearly three times more understaffed, proportionally, than urban American healthcare. And it is getting worse in many regions, not better.
The reasons are well understood at this point. Rural areas pay less, offer fewer career development opportunities, have less social infrastructure for young professionals, and provide limited housing options. The facilities are smaller, the acuity is often high because patients lack access to preventive care, and the professional isolation – not being surrounded by a peer community of nurses – is real.
For a specific type of nurse, rural practice is genuinely compelling. The scope of practice is broader. The relationships with patients are longer and deeper. The advancement timelines can be faster because you are a larger contributor in a smaller system. And for nurses who qualify for federal loan forgiveness programmes tied to working in Health Professional Shortage Areas, the financial picture – when you account for both salary and loan relief – can be competitive with urban salaries after three to five years.
This is not a pitch for everyone to move rural. It is a clear-eyed description of who the rural market genuinely suits and what it offers. If you are a nurse who grew up in a small town and wants to go back, or someone who genuinely values the breadth of rural practice, the opportunity cost of ignoring this market right now is substantial.
What This Means If You Are Thinking About Relocating
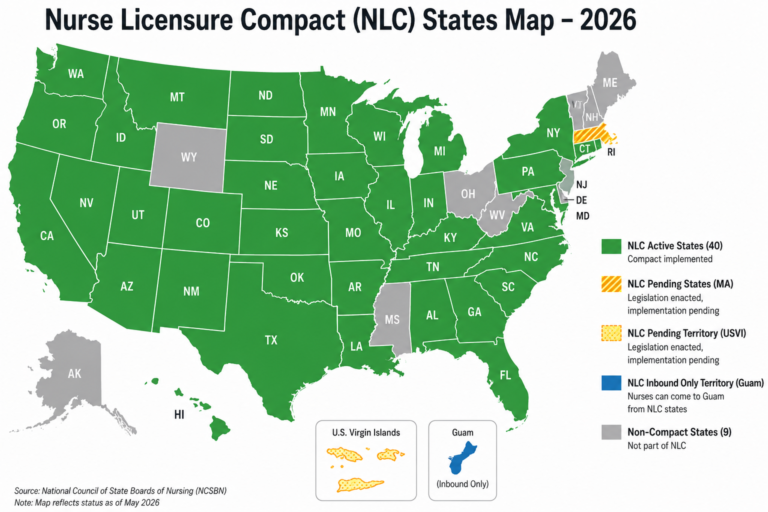
The Nurse Licensure Compact (NLC) currently covers 41 states, meaning nurses with a multistate licence can work across member states without obtaining separate licences for each. This significantly reduces the friction of geographic mobility for most nurses.
If you hold a compact licence and are considering a move – or a travel nursing assignment – the states with the most acute shortage conditions and the most active hiring right now are: California (highest absolute need, strongest pay), Georgia (aggressive metro hiring, strong sign-on packages), Texas (large market, no state income tax), Idaho (highest shortage rate, federal loan forgiveness opportunities), and North Carolina (worsening conditions creating new leverage for incoming nurses).
Before making any decision based on geography, there are four questions worth answering for each state you are considering.
First, what is the actual take-home pay, not the headline salary, accounting for state income taxes, cost of living, and any sign-on bonus repayment requirements? A $30,000 sign-on bonus that comes with a three-year repayment obligation is a fundamentally different financial instrument than one with an 18-month obligation.
Second, what are the staffing ratios at the specific facility? State-level data tells you the market; facility-level conditions tell you your actual workday. These can differ dramatically within a single metro area.
Third, does the facility have Magnet designation, or is it actively pursuing it? Magnet hospitals have a documented track record of better nurse working conditions, stronger professional development investment, and higher nurse satisfaction. If you are BSN-prepared or working toward it, Magnet facilities are worth targeting specifically.
Fourth, what education benefits does the employer offer? In a market this competitive, tuition reimbursement for RN-to-BSN or MSN programmes is increasingly standard rather than exceptional. Negotiating this before you sign – rather than discovering it exists after – puts you ahead.
[→ Related: How to negotiate your nursing salary in a shortage market – a practical guide for 2026]
The Education Credential Factor
There is one pattern consistent across every high-demand state right now that is worth naming directly: BSN-prepared nurses are in a measurably stronger negotiating position than ADN-prepared nurses, even in markets where both credentials are actively recruited.
Magnet hospital hiring policies, clinical leadership tracks, and graduate school eligibility all favour the BSN. The states experiencing the sharpest shortages are also the states where healthcare systems are most actively investing in workforce development – and those investments are disproportionately directed at nurses who already hold or are actively pursuing a BSN.
In 2026, Texas and Nevada frequently rank near the top for nursing salary value once cost of living is applied, and joining an internal float pool is often the fastest way for nurses in these states to reach six figures without relocating. Internal resource pools – where large hospital systems staff their own internal travel positions rather than using external agencies – are becoming the standard strategy at major systems like HCA, Kaiser, and UPMC. These positions typically require or strongly prefer a BSN.
If you are currently practising with an ADN and looking at the states in this article as potential career moves, the decision about whether to pursue your BSN should be made in parallel, not sequentially. The credential matters more in competitive state markets than in the smaller facilities where most ADN-prepared nurses land their first positions.
[→ See our guide: Best Online RN-to-BSN Programs of 2026 – What Working Nurses Need to Know]
A Practical Framework for Reading Your State’s Market
If your state was not specifically covered above, here is how to assess it yourself using publicly available data.
Start with HRSA’s Nursing Workforce Projections report, which provides state-by-state supply and demand figures through 2038. This is the primary government source and the most credible long-range picture available.
Then look at your state’s Board of Nursing annual report, which typically includes current licensure data, exam pass rates, and workforce distribution information. Most states publish these annually.
Finally, look at current job postings – not to count them, but to read them. The language in postings tells you a great deal about how competitive the hiring environment actually is. Markets with excess supply will be more selective in requirements, ask for more years of experience, and rarely include sign-on bonuses. Markets with acute shortages will post urgently, broaden their minimum requirements, include relocation packages, and mention bonuses prominently.
The market is telling you where it needs you. Reading it clearly is a professional skill just like any other.
The Bottom Line for Spring 2026
The nursing job market this spring is the strongest it has been in a generation – but it is not evenly distributed, and the opportunities are not equally accessible to every nurse in every situation.
The nurses positioned best right now are those who hold a BSN, have specialty certification in a high-demand area, hold a compact licence that permits multi-state practice, and are willing to have an honest conversation about geography. That last point matters more than many nurses realise. The shortage is acute in specific places, and showing up in those places – even temporarily, through travel nursing – is one of the most direct ways to convert current market conditions into lasting career momentum.
The nurses positioned least well are those who are waiting for the right opportunity to come to them. In a market this active, with this much geographic variation, the nurses who win are the ones who understand the landscape and move toward it deliberately.
This shortage will ease eventually. History says it always does. But the next few years represent a window of unusual leverage for nurses who understand where the demand is and position themselves to meet it.
National Nurses Week 2026: What “The Power of Nurses” Really Means for Your Career
Is an RN-to-BSN Worth It in 2026? What the Salary and Career Data Actually Shows
Nursing Specialties That Pay the Most in 2026 – And Have Jobs Open Right Now
How to Use the Nurse Licensure Compact to Work Across State Lines in 2026
Sources: Health Resources and Services Administration (HRSA) Nursing Workforce Projections Report · U.S. Bureau of Labor Statistics Occupational Outlook Handbook · Nightingale College 2026 Nursing Shortage Analysis · IntelyCare US Nursing Shortage by State Report · Vivian Health 2025 Nursing Shortage by State Analysis · Atlanta Journal-Constitution Georgia Nursing Shortage Coverage · Deseret News National Nursing Shortage Report, March 2026
Thinking about making a move this spring? [Browse nursing career resources on GlobalNurseGuide →]
Author

Discover more from Global Nurse Guide
Subscribe to get the latest posts sent to your email.